
I Cannot With This I-CAN Plan
Making sense of the new Needs Assessment model

The NDIA announced recently that their new Needs Assessment process is one step closer.
Based on feedback from the disability community that the current way of developing NDIS plans is inconsistent, this major shift will move us from participants supplying their own allied health assessments/reports toward a more standardised (and NDIA-led) assessment tool done by NDIA employees who will be known as ‘Needs Assessors’.
Source: https://www.ndis.gov.au/news/10536-statement-myefo-funding
Former NDIA chief executive Rebecca Falkingham, who left her post last year, originally told Senate estimates in February 25 that allied health professionals should be freed up to deliver services rather than write reports stating “To be really frank about it, my staff can’t read the 280-page reports that they get. They can’t do that in a dedicated kind of way. What we are moving towards is a streamlined support needs assessment tool. It negates the need for all of those reports”
Needs Assessments will be the new way that the NDIA determines what a persons NDIS budget and plan should consist of when we move into the new planning process. This process will be known as ‘New Framework Planning’. Right now we are all still in what’s being referred to as the ‘Old Framework Planning’ system.
Yes you read that right - while we are still lagging way behind the deadline to move participants into the new computer system PACE, we are also rolling out an entirely new way of developing NDIS plans.
Following standard operating procedure NDIS participants heard about the new tool first from the media, followed by an announcement on the NDIS website on 25/09/25. More recently the NDIA announced that this process needs more work and the rollout has now been delayed stating “Following consultation with people with disability and their families, carers and advocates, the rollout of new framework planning will be delayed until 1 April 2027.”
The tool is known as the Instrument for Classification and Assessment of Support Needs (I-CAN) version 6 and it will be used with participants aged 16 and older alongside other questionnaires. The interview to determine an NDIS participant’s needs will be in person and up to three hours long. Additional targeting assessments will also be used for people with more complex needs. This tool is already used by the Dept of Health for Disability Support for Older Australians (DSOA) Program.
The NDIA state that the selection of this tool was supported by a disability lived experience expert advisory group although they haven’t clarified which advisory group that was or what consultation took place.
The University of Melbourne has partnered with the Centre for Disability Studies (CDS) to work with the NDIA in how to modify this tool to ensure it is ‘fit for the purpose’ of Needs Assessments under the NDIS. The tool is conceptually based on the World Health Organisation’s International Classification of Functioning, Disability and Health (ICF), and maps a person’s support needs to 12 domains;
Mobility
Domestic Life
Self Care
Community, Social & Civic Life
Communication
Learning & Applying Knowledge
General Tasks and Demands
Life Long Learning
Interpersonal Interactions & Relationships
Behaviours of Concern
Mental & Emotional Health
Physical Health
Each domain is then broken into four sub-domains except for physical health which has 10 sub-domains.
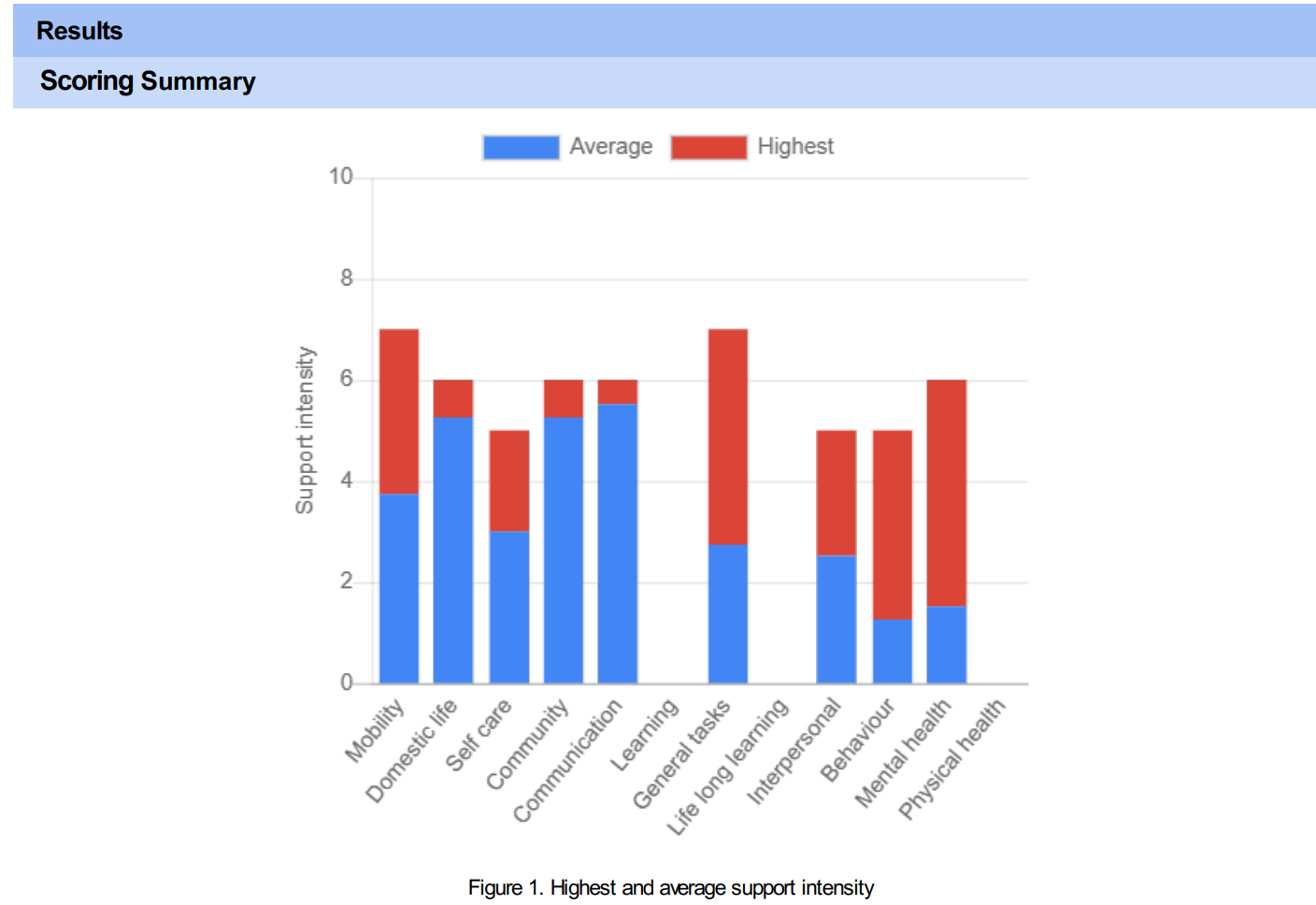
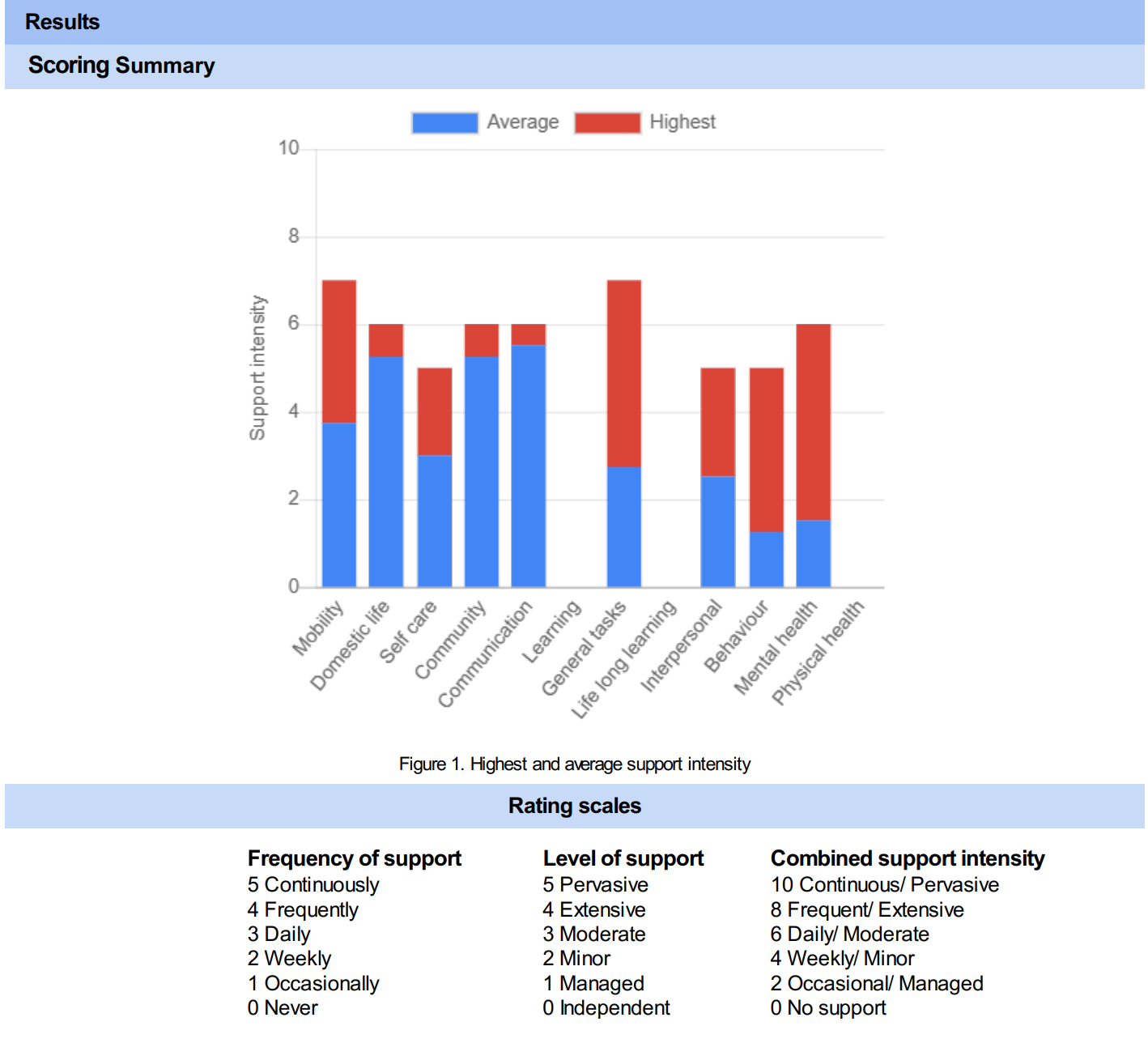
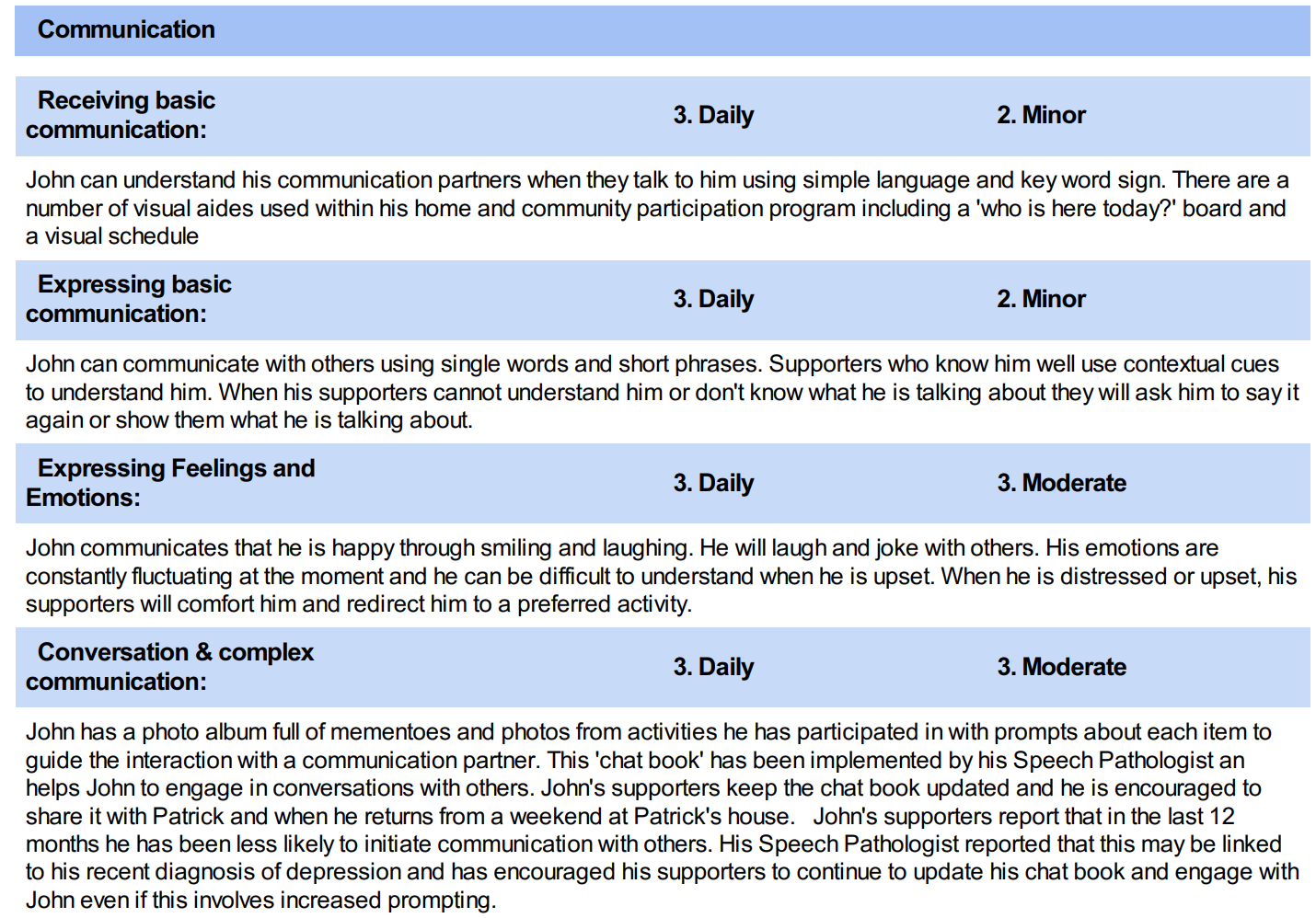
The ICAN has been described as a tool that measures support needs providing a score of the frequency of support needed in each life domain rather than focussing on deficits. It generates a report that shows the frequency of support needed in each domain along with the level of support needed. Those two scores are combined to develop a score for support intensity (see attached screenshots from sample report).
According to The Centre for Disability Studies the I-CAN v6 is a holistic tool that can only be used by trained and certified I-CAN assessors, and training is available to an OT, Physiotherapist, Speech Pathologist, Social Worker, Dietitian, Psychologist, Exercise Physiologist, Rehabilitation Counsellor, Counsellor, Psychotherapist, Registered nurses (RN), Enrolled nurses (EN), Clinicians with an Education degree and NDIS Behaviour Support Practitioners. Other people who feel they have the relevant skills may request to get accredited on a case by case basis.
Currently to administer the I-CAN, a person must access and complete a self-paced online learning program costing $655. They must submit a completed assessment for review and feedback to become accredited within a 6 month timeframe. They then have a license to use the tool for 12 months after which they need to watch a 20 minute webinar and a complete a Re-Accreditation Quiz to extend their licence another 12 months.
CDS Factsheet for I-CAN advises that the tool contains a lot of questions, and that providing background information or reports can help reduce the duration of the assessment.
Let’s look at some example reports from a completed assessment example:
The Legislative Shift
A participants budget in NDIS 2.0 is made up of two powers; Section 32 and the updated 32k.
1/ the supports needs assessment (report created by the assessor) Your support needs are assessed through this process.
2/ that report is returned to the Agency and the bill says that the needs assessment report is applied according to a method applied by the minister.
We don’t have the detail on what that “method” looks like yet.
Which is slightly awkward, given this is the part that actually determines what ends up in the budget.
The Big Question:
Is this Independent Assessments 2.0 with a new haircut?
Is this the return of Independent Assessments that were shut down super fast by the disability community back in 2021. In his original announcement, then Minister for NDIS Bill Shorten was at pains to tell us repeatedly no - and his argument continually hinged on the fact that Independent Assessments would use some form of algorithm to determine support needs, and that Support Needs Assessments will be conducted by a human.
But let’s also consider, Independent Assessments would have at least been performed by an independent party - now we have Assessments being performed by staff hired by the NDIA. It’s like your child’s basketball game being refereed by the other teams coach who also wrote the rulebook and owns the court.
The Glaring Paradox: “We’re not qualified to describe our kids’ needs… unless it’s on an I-CAN form (apparently).”
For many it feels like the NDIS already dismisses or downplays evidence from our own specialist, skilled, qualified, and regulated allied health professionals. We are now being told that the NDIA are flipping to a model that leans heavily on participant/carer self-report via questionnaires after years of being told we need assessments, data and evidence that can only be provided by qualified clinicians.
So why would they suddenly take participant or carer input seriously if it comes from a self-report questionnaire?
Parents and carers are often told we’re not qualified to know what our children’s support needs are. Carer statements can be treated as near-worthless, no matter how detailed or accurate, which makes it hard to believe that this new model will magically start valuing our voices. Parents can absolutely describe their child accurately, but the NDIA has spent a decade telling us we’re unqualified. Are those same voices now considered reliable simply because they’re being channelled through the I-CAN?
And saying the quiet part out loud: a self-report questionnaire can be manipulated. Parents can overstate or understate needs depending on what they believe will produce the best outcome. Which raises the obvious question:
what other information other than the I-CAN will be used to determine the support budget.
The Personal and Environmental Circumstances Questionnaire
The I-CAN tool may be the headline act, but it is not the whole show.
The Support Needs Assessment will also include a Personal and Environmental Circumstances Questionnaire, or PECQ, because we know that no NDIS reform is complete without another acronym entering the chat.
The PECQ appears to be the part of the process designed to capture context that doesn’t fit into neat little tick boxes. The messy human stuff around a participant’s life, including informal supports, changing life stages, goals, risks and safeguards. Whether it does that well is, of course, the bit we will all be watching with our little trauma-informed binoculars.
So will this change make this better or worse…?
As expected plenty of people are lining up to throw tomatoes at this concept. Change is confronting, especially the way the NDIA approaches it with a media drop and zero details.
Firstly a reminder that this new planning framework will only apply to participants aged 16 years or older. For children and young people there have been zero announcements so we can assume (and hope) that for now we still have more control and input into how plans are developed and rightly so.
Childhood development doesn’t follow a straight line, and support needs can shift quickly.
This process is already being tested and trialed. I have seen anecdotal evidence from some saying it was a very positive experience and for others not so much.
Yet for some participants, this genuinely will be an improvement.
Particularly for people with really complex situations, limited informal supports, or who just don’t have the time, money or knowledge to navigate the system and pull together the “right” evidence.
That includes a lot of CALD families, people who aren’t well connected into services, or anyone who’s ever tried to figure out what report they need, who’s allowed to write it, and how to pay for it… and quietly given up.
Right now there are people who should be getting more or different support and the system is too complex with too many barriers for that to occur.
For some getting the right outcome can depend far too much on how well you understand the system, who you’ve got in your corner, and whether you can afford to pay for reports or even find a therapist to write them.
So a more structured assessment process could take some of that pressure off. It could give people a clearer entry point without needing to become a part-time case manager just to be heard.
But that doesn’t mean it’s an improvement across the board.
In the real world, the same structure that helps some people access support can make it harder for others whose needs don’t fit neatly into a standard process.
The Positives:
Having a plan assessment isn’t contingent on having the funding to pay for it
Less conflict of interest from therapists providing reports that they may financially benefit from
Less NDIS funding being used for therapy reports (the may not even be read) and more allied health freed up to work face to face with participants
Less potential for companies to charge ‘one size fits all’ 15 hours for a Functional Capacity Assessment that actually took them 7 hours
Less reports copied and pasted directly from AI
Less variability in quality or format of reports which can vary widely
The Concerns:
The assessment process is now completely controlled by the NDIA who have a clear focus on fiscal sustainability and cost cutting. How is that not a conflict of interest?
Standardised tools are good for consistency, but humans don’t present in standard ways. Complex needs, fluctuating conditions, and overlapping diagnoses don’t always translate neatly into structured assessments.
Instead of government paying qualified clinicians to assess need, the burden shifts onto participants/carers to advocate for themselves through a questionnaire process, potentially often without professional backup.
Assessments are a snapshot. They don’t show how someone’s needs have changed over time, what’s already been tried, or what actually worked. That kind of longitudinal context usually comes from lived experience and therapists who know the person. A one-off assessment tool can’t really replicate that.
The process relies on the availability and timing of NDIA assessors. If there are delays or bottlenecks, (which let’s face it is already an issue) participants may be left waiting for reassessment while their needs change in real time.
Less nuance and richness from reports written by clinicians who know the participants well
Will therapy budgets be reduced now that reports are ‘not needed’?
If a participant disagrees with the report from the assessment tool, their only recourse is to request another Support Needs Assessment
The budget decision is not contestable under this legislation. Participants still have the right to an internal review, but that review will mean another Support Needs Assessment - it does not look at the budget at all.
The good news and the bad news is that this system will still, to some extent, hinge on how well someone can articulate what’s going on and their ability to self-advocate.
It’s really an extension of something we’ve known for years: disadvantage tends to compound. And so does privilege.
My Burning Questions
Here are the questions I’d like some more information about:
Will the Needs Assessment be used to determine AT funding and Reasonable & Necessary, or will allied health reports still be required for equipment?
Will this tool be used for eligibility assessments, or only for plan reassessments?
How can a whole-of-person support budget be generated when legislation limits funding to needs arising from eligible impairments?
If your total budget is non-contestable, how do you challenge decisions about individual supports without reopening the entire budget for review?
How do you appeal for one slice of the pie without risking the whole pie being cut back?
How will Reviews and Appeals work?
We need more information. (I know.)
From what we can tell so far, it looks like everything in the Participant Statement of Supports will be reviewable… but the budget decision itself won’t be.
This is where a lot of the concerns lie. Right now the right to review is a strong protective factor for participants who don’t fit into a neat box. External reviews particularly so.
Case in point;
If your budget is determined as a single figure based on the assessment outcome, how do you challenge one part of it?
For example, if you’re comfortable with your Core supports but disagree with the level of therapy funding, how do you isolate that decision when it’s all been rolled into one total budget?
At this stage, it doesn’t look like you can.
Instead, if a participant seeks a review, whether internally or through the ART, the process appears to trigger another Support Needs Assessment. Potentially with a more experienced assessor.
And then the same “method” (that we still haven’t seen) is applied again to produce a new budget.
This is one of the main concerns of the disability community, and rightly so.
If too many reviewable decisions are clustered together in one total support budget and when you request one part of the ‘pie’ to be appealed, you open up the whole pie to be reviewed.
Then what?
In Summation…
At this stage, there are still more questions than answers. Some parts of this reform could make things easier or fairer. Others may introduce new risks that aren’t fully understood yet.
Like most things in the NDIS, the detail will matter. And so will how it plays out in real life.
For now. if you want to be part of the pool of participants who are testing out the New Framework Planning and give your feedback, you can sign up to Participant First Program here: https://engage.ndis.gov.au/projects/engagement-opportunities-for-the-new-way-of-planning
The timeframes may blow out further, or the NDIA may pivot and completely change to a new process. We’ve seen enough to know that how something is designed and how it actually plays out are often two very different things.
“Nothing is so certain as the unexpected.” — Alice Walker
Until next time;
x Anna